

- The One Idea That Explains Almost Everything
- What Actually Happens, and When
- Nausea and Vomiting: Eating for a Slow Stomach
- Constipation and Diarrhea: The Slow Clock at the Other End
- The Symptoms Nobody Quite Warns You About
- When It’s Not Just a Side Effect
- Slower Beats Quitting
- Frequently Asked Questions
- How long do GLP-1 side effects last?
- Does the timing or technique of the injection change side effects?
- Do GI side effects mean the medication is working?
- Does one GLP-1 cause fewer side effects than another?
- Can I take anti-nausea or anti-diarrhea medicine alongside a GLP-1?
- The Bottom Line
Affiliate disclosure: This article contains affiliate links. We may earn commission when you purchase through partner links, at no extra cost to you. Editorial independence preserved — recommendations based on provider compliance and patient outcomes, not commission rates. This article is informational and is not medical advice.
If you are about to start a GLP-1 medication, or you are a few weeks in and wondering whether what you feel is normal, here is the one idea that makes the rest make sense: the drug has put your stomach on a slower clock. The nausea, the early fullness, the constipation, the reflux — almost every gastrointestinal side effect is a version of that single change. Understand the slow clock and you stop memorizing a list of tips and start reasoning your way through it. This guide does exactly that — what the slowdown feels like, when the hard days come, how to eat so your stomach can keep up, the symptoms nobody quite warns you about, and the handful of signs that mean something other than an ordinary side effect.
The One Idea That Explains Almost Everything
GLP-1 medications — semaglutide in Ozempic and Wegovy, tirzepatide in Mounjaro and Zepbound — were not designed to upset your stomach. They were designed to slow it down, and the upset is the slowdown showing itself.
These drugs work in two places. In the brain, they act on the regions that govern appetite — and those regions sit right next to the ones that govern the nausea reflex, which is why reduced appetite and queasiness so often arrive together. In the gut, they slow the rate at which the stomach empties and the rate at which everything moves through the intestines. That delayed emptying is the entire point: food lingers, you stay full longer, you eat less. But a stomach that empties slowly is a stomach with a smaller working capacity and a longer to-do list, and when you feed it as though nothing has changed, it pushes back — as heaviness, as nausea, as reflux when there is simply no room. Slow the intestines and the far end of the system slows too, and that is constipation in a single sentence.
So the side effects are not a glitch. They are the visible edge of the mechanism that makes the drug work. That is genuinely useful to know, because it means they are predictable, they respond to how you eat, and for most people they ease as the body recalibrates around the slower clock.
What Actually Happens, and When
The intensity of GLP-1 side effects is not spread evenly across the months — it tracks the dose. These drugs are titrated deliberately: you start low and step up every few weeks, and that schedule exists precisely because the gut needs time to adjust to each new level.
The pattern most people experience runs like this. The starter dose is usually the gentle introduction — some queasiness, perhaps a shift in bowel habits, nothing dramatic. The hard days come after each step up. For many people the worst of it lands in the first one to three days after a dose increase, then fades over the following week or two as the body settles at the new level. By the second month the floor tends to rise: the symptoms become less frequent and less sharp, and once you have held the maintenance dose for a while, most of it has quieted to something minor or gone.
Two practical things follow. First, a wave of nausea two days after a dose increase is the system behaving exactly as expected — not a sign the drug is wrong for you, and usually gone within the week. Second, because the rough stretch is semi-predictable, you can plan around it: keep the day or two after a step-up light and undemanding, and some people deliberately take their injection in the evening so they sleep through the worst of it. The pattern that does not fit — brand-new gastrointestinal symptoms appearing for the first time many months into a stable dose — is the one worth getting checked.
Nausea and Vomiting: Eating for a Slow Stomach
Nausea is the symptom people most want gone, and the single most effective lever is not a medication — it is matching how you eat to the stomach you now have. Two things overwhelm a slow stomach: volume and fat. A large meal hands it more than it can process. A fatty meal empties slowly even in a normal stomach, and on a GLP-1 that becomes the classic trigger for nausea and outright vomiting. Fried food, creamy sauces, cheese-heavy dishes, a big cut of meat, pastry — these are the reliable offenders. So are a few things people do not expect: the large coffee on an empty stomach, the morning protein shake knocked back in one go, the “healthy” salad drowned in oil. The foods are not the problem in themselves; the problem is that they ask too much of a stomach running slow.
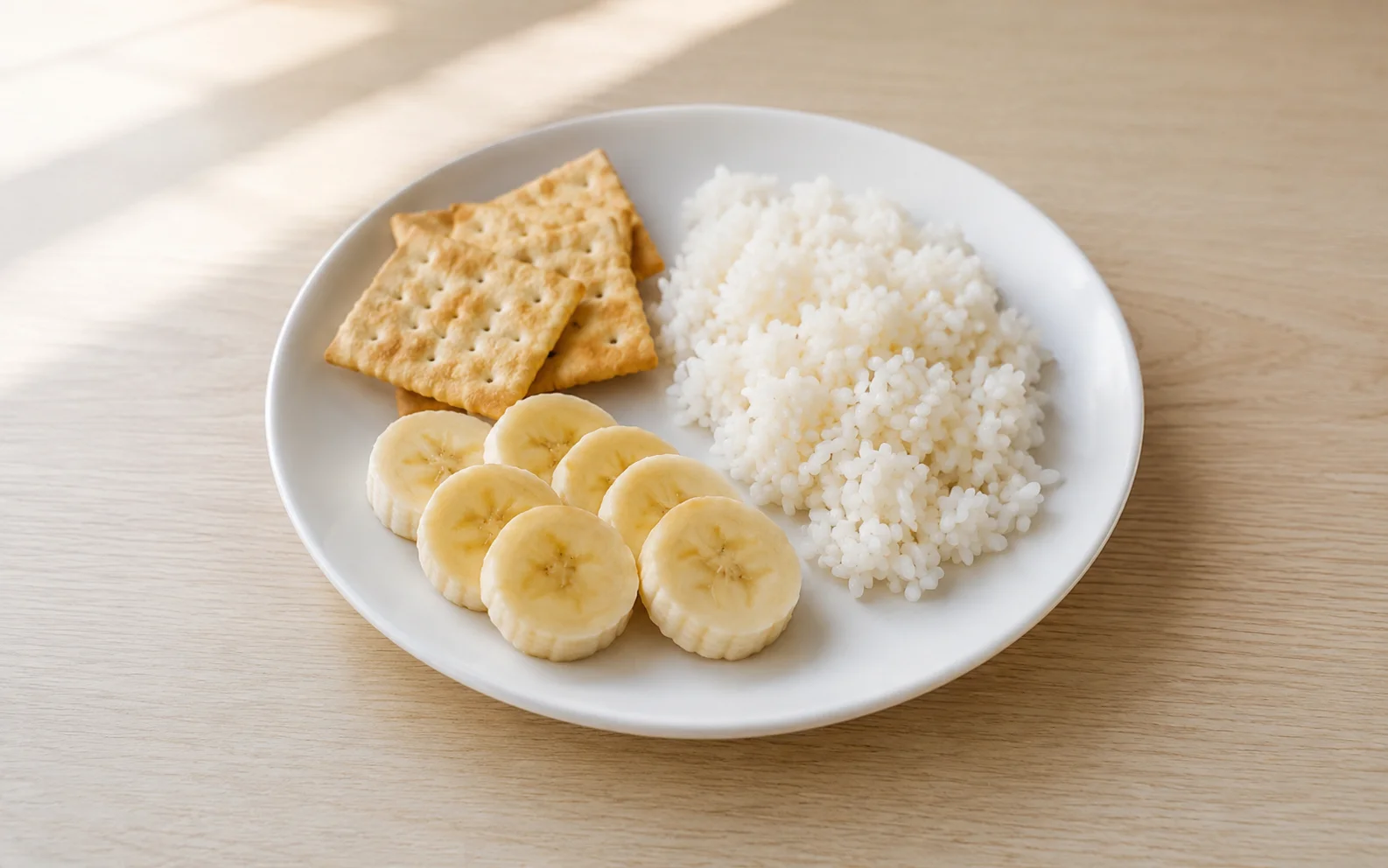
The fixes follow directly. Eat smaller amounts more often, so the stomach is never holding more than it can move. Keep meals on the plainer, leaner side — the standard nausea foods, plain rice, toast, crackers, bananas, lean protein, are not a cliché, they are simply low in volume and low in fat. Eat slowly, because fullness on a GLP-1 does not arrive gently. It tends to hit as a wall: you are eating normally and then, within a bite or two, you are completely and abruptly done. Pushing one more bite past that wall is the single most common self-inflicted cause of vomiting there is, and learning to stop just before it — rather than at it — is a real skill worth practicing. Stay upright for a while after eating instead of lying down, which eases both nausea and reflux. Sip fluids steadily through the day. Ginger, as tea or otherwise, is a genuine low-risk option that settles many stomachs.
When eating well is not enough, the next moves belong to your prescriber, and they are worth asking for rather than enduring a miserable fortnight: slowing the titration, holding longer at the current dose before the next step, or a short course of anti-nausea medication to cover a bad patch. Vomiting that will not stop is a clear reason to make that call — past the misery, it drains you toward dehydration quickly.
Constipation and Diarrhea: The Slow Clock at the Other End
Constipation is the side effect that does not read the timeline. Where nausea tends to fade, constipation can settle in and stay, because the same slowed transit that keeps you full is, further down, simply a slower colon. The mistake is waiting for it to pass on its own. Treat it from the start: build up fiber gradually — vegetables, fruit, whole grains, prunes, chia — drink genuinely enough water, since fiber without fluid makes a hard problem harder, and keep moving, because physical activity moves the bowel along with it. If that is not enough, a gentle over-the-counter laxative or stool softener is a normal and reasonable next step, and a pharmacist can match one to you.
Diarrhea is the opposite problem and usually the shorter-lived one. It tends to show up early, as the gut adjusts to the change in transit, and often settles on its own within a few weeks. While it lasts, the priority is fluid and electrolytes, which diarrhea strips out fast, alongside plain, simple food. The version that is not ordinary — diarrhea that is severe, bloody, or simply not stopping — needs medical attention rather than patience.
The Symptoms Nobody Quite Warns You About
The nausea and the bowel changes are well advertised. A few other effects are real, common enough, and oddly missing from most briefings — and knowing they are normal spares you a lot of needless worry.
The first is burping, often with a sulfur smell — a genuine rotten-egg quality that is as unpleasant socially as it sounds. It is tied to slowed digestion and tends to be worse after fatty or heavy meals, which means the same smaller, leaner meals that ease nausea usually quiet it too.
The second is a change in your relationship with food itself. GLP-1 drugs do not just shrink appetite; for many people they turn down “food noise” — the background hum of wanting, planning and thinking about food. That is often welcome. It can also be disorienting: foods you genuinely loved can become flatly unappealing, and meals can start to feel like a chore. The practical consequence is that you have to eat with some deliberateness rather than waiting to feel like it — protein especially, because losing weight while skimping on protein costs you muscle you do not want to lose.
The third is quiet and easy to miss: thirst fades along with appetite. The same signaling that dampens hunger can dampen thirst, so people on GLP-1s routinely drink too little without noticing — which then resurfaces as worse constipation, more fatigue, and a washed-out, faintly queasy feeling that is really mild dehydration. Drinking on a schedule rather than waiting for thirst is a small habit that heads off a surprising amount of trouble. Fatigue itself is common too, particularly in the early weeks and after dose increases; part of it is simply that you are eating considerably less, and it usually lifts. Fatigue that is severe or unrelenting, though, deserves a look — it can flag inadequate nutrition or dehydration rather than the drug alone.
When It’s Not Just a Side Effect
Everything so far is the ordinary, expected range — unpleasant, manageable, temporary. A smaller set of symptoms sits outside that range, and these mean getting medical help promptly rather than waiting them out:
- Severe, constant abdominal pain that bores through to the back. Pancreatitis pain is distinctive — not a cramp that comes and goes, but a relentless, intense pain high in the abdomen that often radiates straight through to the back and comes with vomiting. It is rare, but it needs urgent evaluation.
- Pain in the upper-right abdomen, sometimes with fever. This points toward the gallbladder — gallstones or inflammation — a recognized risk with this drug class.
- Vomiting that will not stop, or being unable to keep any fluid down. Beyond being unbearable, this leads to real dehydration, and can occasionally signal that the gut has slowed too far.
- No bowel movement for a long stretch, with a swollen, distended abdomen and vomiting. That combination can mean a bowel obstruction and should be assessed without delay.
- Signs of dehydration — dizziness, a racing heart, very dark urine, marked weakness — particularly after a run of vomiting or diarrhea.
Two points beyond the symptom list. GLP-1 medications carry the FDA’s strongest class of warning — a boxed warning — over a possible risk of thyroid C-cell tumors seen in rodent studies; they are not for people with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2. And watch the scale, not only your stomach: weight dropping extremely fast, or feeling persistently drained and unable to eat properly, is itself worth raising. Losing weight far too quickly is a problem to flag, not a result to celebrate.
💊 Looking for a Lower-Cost Compounded Option?
For cash-pay patients, compounded semaglutide is a lower-cost compounded option through a clinician-supervised telehealth model. Direct Meds offers Summer 2026 promotional pricing:
- Compounded Semaglutide: $147 first month ($150 OFF regular $297)
- Clinician-supervised dosing and titration support
- 503B compounding pharmacy network — patient-specific prescriptions
- LegitScript-certified telemedicine compliance
- USP <795> and USP <797> sterile compounding standards
- Available in 48 states (excludes MS and LA)
Compounded semaglutide contains semaglutide, but the compounded product itself is not an FDA-approved finished product and is not reviewed by the FDA for safety, effectiveness or quality. Whether it is appropriate for you is a decision for you and your clinician.
Slower Beats Quitting
Gastrointestinal side effects are the most common reason people walk away from GLP-1 treatment — by some real-world estimates around a quarter of patients stop within the first year, GI symptoms prominent among the reasons. A great deal of that is avoidable, and it comes down to one misconception worth dismantling: that the choice is between toughing out the prescribed schedule and giving up.
It is not. The schedule is not sacred. If a dose step is genuinely intolerable, the sensible move is to slow down — hold longer at the dose you tolerate, step back down a level, or stretch out the climb — and the drug does not punish you for it. Reaching the maintenance dose over eight months instead of four does not make it work any less well; it just means you got there in a way you could live with. That is a conversation to have with a prescriber rather than a change to make alone, since a dose decision is a clinical one and stopping outright carries its own consequence — appetite, and usually weight, tend to return. But the message to bring is simple: this is hard, help me slow it down. A good prescriber would far rather adjust the climb than lose you from treatment altogether.
Frequently Asked Questions
How long do GLP-1 side effects last?
For most people the common symptoms are worst at the start and in the days after each dose increase, then ease over the following weeks — many notice clear improvement within the first one to two months. Constipation can outlast the rest. Symptoms that stay severe, or are not improving after several weeks at a steady dose, are the exception worth getting checked.
Does the timing or technique of the injection change side effects?
The dose drives side effects far more than the timing does, but timing can still help you cope. Because the roughest stretch tends to fall in the first day or two after a step-up, some people take their weekly injection in the evening so the worst of it passes while they sleep. There is no single “correct” day or time — pick a consistent slot that fits your week, and keep the day after a dose increase light.
Do GI side effects mean the medication is working?
No. The intensity of side effects does not track how well the drug is controlling blood sugar or driving weight loss. Plenty of people get strong results with only mild nausea, and a rough start does not predict a better outcome. Side effects and effectiveness are separate things — there is no reason to tolerate worse symptoms in the belief that they signal success.
Does one GLP-1 cause fewer side effects than another?
All GLP-1 medications share a similar gastrointestinal side-effect profile, and individual response varies more than the gap between drugs. Some research suggests modest differences between agents, but none is reliably “gentle” for everyone — dose level and titration speed matter more than brand choice. If one medication is genuinely intolerable, switching to another is a reasonable option to raise with a prescriber.
Can I take anti-nausea or anti-diarrhea medicine alongside a GLP-1?
Often yes. A pharmacist can point you to an over-the-counter option that suits you, and a prescriber can supply an anti-nausea medication for a hard titration step. The reason to ask first is simply to make sure the choice fits the rest of your medication list.
The Bottom Line
Almost everything your stomach does on a GLP-1 traces back to one change: it is running on a slower clock. Feed it accordingly — smaller, leaner, slower, with fluid and fiber kept up deliberately — and the common side effects are mostly a manageable early phase that fades as your body recalibrates. Keep the titration as gentle as you need it, because a slow climb you can tolerate beats a fast one you abandon. And hold one short list apart from the ordinary discomfort — relentless abdominal pain, unstoppable vomiting, signs of obstruction or dehydration — as the symptoms that mean help, now. For how the individual drugs compare, see our 2026 brand comparison; for what they cost, our GLP-1 cost guide.
Considering a Compounded Option?
For cash-pay patients pursuing semaglutide, Direct Meds offers compounded semaglutide through a clinician-supervised telehealth model, with Summer 2026 promotional pricing:
- $150 OFF first month compounded semaglutide injection ($147 vs regular $297)
- Licensed clinician reviews eligibility and oversees dosing and titration
- 503B compounding pharmacy network — patient-specific prescriptions
- LegitScript-certified telemedicine compliance
- USP <795> and USP <797> sterile compounding standards
- Telemed evaluation included (typically $99 value), 1-2 day FedEx/UPS shipping
- Available in 48 states (excludes MS and LA)
180,000+ patients have used Direct Meds; current Trustpilot rating 4.8. Compounded semaglutide contains semaglutide, but the compounded product itself is not an FDA-approved finished product and is not reviewed by the FDA for safety, effectiveness or quality. Whether it is appropriate for you is a decision for you and your clinician.
Affiliate disclosure: allcheminfo.com receives commission when readers start treatment through Direct Meds. Recommendation based on their 503B pharmacy partnership, LegitScript certification, and clinician-supervised model — not commission rate.
Clinical details in this article reflect publicly reported information as of May 2026 and are general in nature. They are not a substitute for individual medical advice — discuss any side effect, dose change or new symptom with a licensed clinician.



